GLP-1 agonists have transformed obesity treatment with evidence of significant weight loss and benefit in weight-related comorbidities. However, cost and insurance barriers limit patient access, and coverage changes may make obtaining a GLP-1s for weight loss even more challenging in the future. Even for those with affordable coverage, injectable administration and GI side effects may still deter use, necessitating consideration of alternative AOMs. All AOMs are indicated as adjunct treatment alongside a reduced-calorie diet and lifestyle modifications. Of note, Medicare does not cover any medication for the treatment of obesity, including oral AOMs.
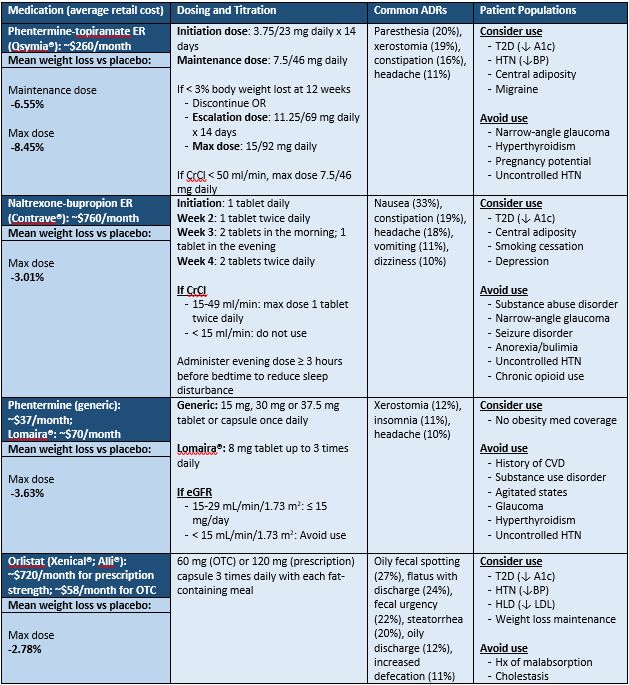
Phentermine-topiramate ER (Qsymia®) is currently the most effective oral AOM, but does require dispensing pharmacy certification in the Qsymia® REMS program due to the teratogenic risk of topiramate. As a stimulant, phentermine-topiramate ER should be avoided in those with a history of cardiovascular disease (CVD), substance use disorder, agitated states, glaucoma, hyperthyroidism, or uncontrolled hypertension (HTN). Generic phentermine-topiramate ER became available in May of 2025, the cost and availability impact of this is to be determined. For those without insurance or inadequate AOM coverage, savings options are available through the manufacturer's website.
Naltrexone-bupropion ER (Contrave®) has moderate efficacy in weight loss and comes at a higher price point than other oral AOMs. Naltrexone-bupropion ER offers an alternative for those with comorbidities that preclude them from using phentermine-topiramate ER. Naltrexone-bupropion should be avoided in those on opioid therapy, those with substance use disorder, narrow angle glaucoma, seizure disorder, anorexia or bulimia, or uncontrolled HTN. Naltrexone-bupropion can be considered for those with obesity who are interested in smoking cessation or those with depression. For those without insurance or inadequate AOM coverage, savings options are available through the manufacturer's website.
Phentermine is generically available and indicated for short-term weight loss only (≤ 12 weeks). Despite its indication in short-term weight loss, it is often used off-label for chronic obesity management in adults without CVD. There are currently no long-term cardiovascular outcome trials for phentermine monotherapy. Of the AOMs mentioned, phentermine is the most affordable and can be considered for patients with cost and coverage barriers with other weight loss medications. Phentermine is available as a low-dose 8 mg tablet under the brand Lomaira®.
Orlistat (Xenical®; Alli®) provides modest weight loss for patients who are unable to tolerate a centrally-acting agent. Due to considerable GI side effects, the American Gastroenterological Association recommends against its use for most patients and adherence is generally poor. Patients taking orlistat should be counseled on taking a MVI with fat-soluble vitamins at bedtime to avoid deficiencies and orlistat should be avoided in those with chronic malabsorption and cholestasis. Orlistat is the only agent with an OTC option (Alli®), although there is limited long-term data on the efficacy of the OTC dose of 60mg.
For combination AOMs which are expensive for patients, prescribing the individual generic components may be more affordable. For additional information on how to do this, please reference this resource.